Colorado Medical Society
http://dev.cms.org/articles/physician-heroes-going-global/Physician heroes: Going global
Wednesday, July 01, 2015 12:26 PM
Larry Kieft, MD, MPH, a retired obstetrician-gynecologist in Fort Collins, has always been interested in access to health care; his philosophy was that all women should have access to care. His former private practice was one of the few in the community at the time that accepted women with no health insurance, with very few resources or with Medicaid coverage. He helped start the Poudre Valley Prenatal Program – which provided prenatal care, delivery and postpartum services for approximately 300 underserved women annually – and he served as the clinical director for 21 years.
“It’s always been part of my heart and desire that women have access to good preventative care as well as safe pregnancies and deliveries, and have a good start for their children,” Kieft said.
So when he heard a report about mother-to-child transmission of HIV in Africa, he embraced a call to service that would lead him around the world to provide OB-GYN care to women and teach indigenous health care providers methods to help prevent maternal mortality.
First lessons
His first trip abroad was to Bangladesh in south Asia to visit medical projects in rural areas and in the slums of Dhaka, the nation’s capitol. “This was important for me to do because I had in my mind that medical care and delivery systems in the developing world were probably like the 1950s [in the developed world]. It was really like the 1850s,” Kieft said.
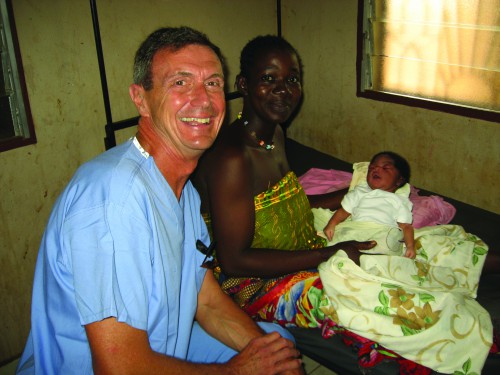
Kieft celebrates a successful delivery with a patient and her newborn baby boy.
The maternal mortality rate in the United States is roughly seven women per 100,000; in the developing world it can be up to 600 women per 100,000. In rural areas in the developing world, there is no ambulance service, there’s no local hospital, and patients may have to walk for a day to reach a center where help is available. Women and babies are dying of what he considered to be preventable causes.
“That was a real wake-up call,” he said. “I realized that health care delivery systems were very complicated in the developing world. Most women who were delivered in rural areas had no prenatal care. Traditional birth attendants did their deliveries but they just learned these skills from other women. They didn’t have access to supplies or equipment so women were dying from results of hemorrhage, infection following a delivery or a miscarriage, or complications of high blood pressure.”
Because of the cultural challenges of a man caring for women in a Muslim country, he refocused on Africa and has since traveled to the countries of Mali, Nigeria, Kenya, Rwanda, Malawi and Zambia, working for a month at a time and searching for the “perfect fit” for his interests and skills. He sought a place where English was one of the primary languages and where he could teach indigenous physicians, which he felt could have more impact than just providing direct care.
Finding a place
His five most recent trips have been to Tenwek Hospital in Kenya, a 300-bed hospital in a rural setting north and west of Nairobi. Providers there deliver 3,000 babies a year; “these are the complicated ones because the normal ones deliver at home,” he said. The hospital has an internship program both for medical interns and physician assistant interns, a nursing school, general surgery residency, orthopedic residency and a permanent medical staff comprised of expats and Kenyans.

Kieft teaches surgical techniques to young physicians in Mali.
“Every time I’ve gone back to the same place, I’m trusted more, people know I’m taking them seriously, and I listen,” Kieft said. “I try to listen to what’s happening and to their goals, not impose my goals for their health or their community. It’s very important that when you deliver medical care in this kind of context that you understand their culture. We cannot just transport our technology to another place and assume it has the same meaning or use.”
Kieft teaches young physicians surgical skills, basic prenatal care so that problems can be recognized before they become catastrophes, and how to manage a woman with a complication during pregnancy. He also focuses on early detection of cervical cancer through a method that uses vinegar and a flashlight: visual inspection of the cervix after acidic acid application, or VIA. Combined with cryotherapy, this approach has been proven successful in the developing world in detecting and treating pre-cancerous lesions in one visit.
“In the developed world, the mortality rate from cervical cancer is about 20 percent once it’s diagnosed. In the developing world it’s 80 percent. The problem is that it’s not detected early, there aren’t any facilities for extended treatment, and all of the technology we would use isn’t available. This type of program, VIA, has shown that if a woman has only two such visits in her life, you reduce her risk of dying from cervical cancer by 40 percent.”
Kieft demonstrates principles of differential diagnosis and prioritization of patients, which are cornerstones of American medical education but not necessarily taught in African medical training.
“These young physicians are very bright,” he said. “It’s not a lack of intelligence; it’s a different style of learning. Our medical education is very hands-on. Theirs is in big lecture halls. As far as treating patients, often what they learn is from other medical students or just by doing. I spend a lot of time with them, do rounds with them, go to clinic with them, discuss how they want to treat a condition, what they want to do. It’s modeling that kind of behavior. I’m very relational in my style of teaching so it goes over very well with these young physicians.”
Another behavior he imparts is the value of women. He shared two quotes of great importance to him:
- “The obstacles that stand in the way of better health for women are not primarily technical or medical in nature but rather social and political.” - Margaret Chen, head of the World Health Organization.
- “Women are not dying because of diseases we cannot treat. They are dying because societies have yet to make the decision that their lives are worth saving.” - Mahmoud Fathalla.
“The status of women is not good in the developing world and their health care is even worse,” Kieft said. “Often they are in a position where they can’t make decisions about their own health care; they need money from their husband, father or brother, and permission to be treated. Economically, the value of a woman isn’t thought of very highly even though there’s all kinds of data showing that women who work enhance the economic wellbeing of the family. So the other thing I try to do is model the value of women and teach that to the interns and residents.”
A way to love medicine again
The work can be emotionally challenging but extremely rewarding. Kieft told a story of the parents of a young woman who died in the operating room. “They started by thanking me,” he said, with traces of tears in his eyes. “They said, ‘we know you tried everything. She was very sick when she got here.’”
“You have to open yourself to that possibility and be able to accept the fact that we can change many things but there are some things beyond our power to change. On the other side, there is great joy: A woman presents with a very complicated pregnancy and you get to deliver a healthy baby. We have that joy here but in the developing world we know it can go another way just as well. That gift of joy is really something. I get so much out of this. It’s good for my spirit.”
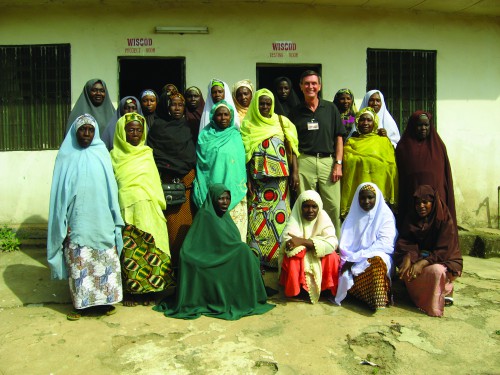
Kieft poses with a group of traditional midwives in Nigeria after teaching a course on postpartum hemorrhage.
Kieft’s passion for his work in the developing world is palpable and he is eager to share information with any CMS member interested in embarking upon a similar journey, particularly retired physicians who are interested in service in the developing world (email him at larrydkieft@gmail.com). “It’s been a great way for me to use my medical skills,” he said. “I really didn’t want to deal with the business of medicine anymore. I loved my patients; I loved practicing. This has allowed me to continue loving medicine, interacting with patients and experiencing things that I’ve always loved, and putting to use the gifts that I have in an area of great need.”
He advises interested physicians to just start talking to others: “let people know you’re considering international medical service. Once you put your name out there, people start feeding you information,” he said. “People are dying, literally dying, for the skills we have. Physicians have good hearts and I think this is a great opportunity to use their passions and skills in an exciting way.”
Editor’s note: The Colorado Medical Society recognizes the prevalence of burnout among physicians. To help our members reflect on the difference they’re making in the lives of their patients and community, and to recognize extraordinary actions, Colorado Medicine presents the Physician Heroes series. We will profile as many different members as we can who have gone above and beyond in the profession to help their colleagues or community. We hope you’ll see your own values reflected in these stories and be reminded of the joy of medicine.
Nominate yourself or a member colleague by contacting Dean Holzkamp at dean_holzkamp@cms.org or Kate Alfano at kate_alfano@cms.org.